Let´s celebrate!. A high impact journal as Intensive Care Medicine, starts talking in What’s new in Intensive Care about the use of physical restraints (PR) in critically ill patients.
Perhaps it could sound rare to affirm that the use of PR is a new issue, but the were no studies or references till very late years ago. It was really difficuld to find articles about this: reading about self-withdrawal endotracheal tubes sometimes the presence or not of PR was registered as a variable, without talking about the type/indication/side effects/other alternative approaches… Really, physical restraints were an almost invisible measure in our enviroment and the magnitude of this problem has been undervaluated.
We think that it´s a milestone that a journal as Intensive Care Medicine considers the use of PR in ICU as a problem, and we defend the reduction and the reflexive management of PR. The article shows clue elements that could be applied in ICU around the world, included Spain. The use of PR is not free of physical and psychological risks, threatens the right of patients and ethical principles of a person.
- ICU could be the last border where the use of PR continues as a daily practice. In Geriatrics or Mental Health are working against the use and the myths since several years. Authors point out the analogy in the beliefs in Geriatrics and ICU: there is no evidence about PR could prevent falls in elderly people (it could ever favor them) and also there is no evidence actually showing the use of PR to prevent self-withdrawal of endotracheal tubes.
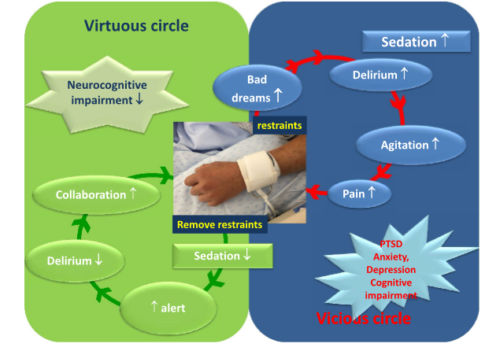
- The use of PR is presented as a vicious circle increasing pain, agitation and delirium. This generates and increasinf of sedation and less patient collaboration. So, an strategy to break this circle could be an scheduled and studied reduction of the use of PR.
- Suggesting that high prevalence of the use of PR is only due to nurse/patient ratios doesn´t seem appropiate, and in many places could be an impossible solution. An adequate nurse/patient ratio could be an element and for sure it should be changed in many cases, but effective strategies to reduce the use of PR should be multiple and directed to a cultural change.
However, in our country the proposed approachs till now have superficials, only centered basically in the presence or not of an institutional protocol without analizing if this protocol is adapted to the ICU needs or the grade of implementation. been. A problem of the complexity and magnitude as the use of PR shoud need deeper reflexions more than the presence or not of a protocol.
So, we are in luck and in front of a big challenge: in the Era of humanisation, conscious sedation, early mobilization, the ABCDEF by Ely and cols., the eCASH concept…at the end person centered care, a high impact journal puts explicitly and finally on the table the use of physical restraints in ICU.
It´s time to work!!!
REFERENCES
- Burry L, Rose L, Ricou B. Physical restraint: time to let go. Intensive Care Med.2017 Nov 23.
- Rubio Domínguez J. Contención mecánica de pacientes. Situación actual y ayuda para profesionales sanitarios. Rev Calid Asist.2017;32(3):172-177.
- López Camps V, García García MA, Martín Delgado MC, Añón Elizalde JM, Masnou Burrallo N, Rubio Sanchiz O et al; Grupo de Trabajo de Bioética de la Sociedad Española de Medicina Intensiva Crítica y Unidades Coronarias. Med Intensiva.2017;41(9):523-531
- Sociedad Española de Medicina Intensiva Critica Y Unidades Coronarias [homepage on the Internet]. Recomendaciones NO HACER de los grupos de trabajo de la SEMICYUC. [citado 12 Dic 2017]. SEMICYUC ; [aprox. 1 pantalla].






{kind=link}
Leave A Comment