On many occasions, the decision-making on the disabled and severely ill patients falls on the family. It is not easy to be in this situation: there are serious problems of communication that generate anguish in the family in the short and long term and can lead to unwanted treatments by the patients, which carry suffering, therapeutic futility and elevated economic costs. Although clinical practice guidelines recommend family support strategies, it is clear that many people who could Benefit do not receive it.
Last week, New England Journal of Medicine published the article A Randomized Trial of a Family-Support Intervention in Intensive Care Units , by the PARTNER (Pairing Re-engineered ICU Teams with Nurse-Driven Emotional Support and Relationship-Building) research group from the Critical Care Department of University of Pittsburgh School of Medicine.
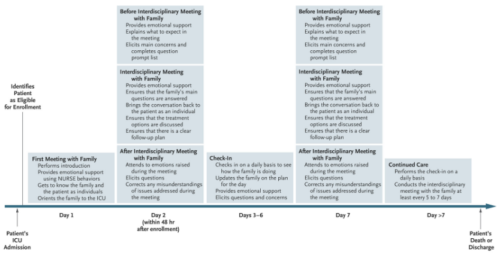
They conducted a stepped-wedge, cluster-randomized trial involving patients with a high risk of death and their surrogates in five intensive care units (ICUs) to compare a multicomponent family-support intervention delivered by the interprofessional ICU (leaded by nurses who received advanced communication training that focused on skills for supporting families of seriously ill patients) with usual care.
The primary outcome was the surrogates’ mean score on the Hospital Anxiety and Depression Scale (HADS) at 6 months.
Prespecified secondary outcomes were the surrogates’ mean scores on the Impact of Event Scale, the Quality of Communication (QOC) scale and a modified Patient Perception of Patient Centeredness (mPPPC) scale, as well as the mean length of ICU stay.
Among the 1420 patients admitted to the study, there were no significant differences between the two groups in the HADS and IES scales at 6 months.
However, the scores of the QOC and mPPPC scale had statistically significant differences in favour of the intervention group. The mean length of stay in the ICU was shorter in the intervention group than in the control group (6.7 days by 7.4), a finding mediated by the shortened mean length of stay in the ICU among patients who died (4.4 days Vs 6.8). The intervention did not affect the average stay in the ICU of the patients who survived.
The authors conclude that an intervention with families (which is also low cost) does not prevent their psychological alterations, but improves communication and care focused on them, shortening the ICU stay compared with the usual treatment.
Often the most obvious thing is the most obviated one. What else do we need?
Here it is, this is Science.






{kind=link}
Leave A Comment