Lancet Respiratory Medicine has just published online the international collaborative research Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): a multicentre cohort. This is a work of the COVID-19 Intensive Care International Study Group, formed by members of Universidad de Valencia and INCLIVA, the Vanderbilt University’s Critical Illness Brain Dysfunction and Survivorship Center and Proyecto HU-CI.
It is probably the article I am most proud of for several reasons:
First, it was developed during the toughest months of the first wave of the pandemic, thanks to the work of many, many people from 69 ICUs in 14 countries put into the service of a good idea. Secondly, because the first authors are the sample of this collaborative work: a nurse co-author with an anesthesiologist in the first place, an intensivist, three statisticians, neurologists, internists… I firmly believe that this is the way things should be and it is a sample of international research for the future: egos are left out because together we are stronger. And thirdly, this is research with most of the patients recruited in Spain.
Working with Vanderbilt University’s Critical Illness Brain Dysfunction and Survivorship Center has been a similar experience to driving a formula 1: a perfectly oiled machine where each person adds his or her talent, pursuing excellence and the best possible result. Sincerely, a lot to learn at your side and unfortunately, I feel that we are light years away from this model in Spain.
Between Jan 20 and April 28, 2020, 4530 patients with COVID-19 were admitted to 69 ICUs. Data were collected from 2088 patients admitted to the ICU with SARS-CoV-2 infection over a 21-day period to assess the prevalence and risk factors for delirium.
The median age of patients was 64 years with a median Simplified Acute Physiology Score (SAPS) II of 40. 1397 of 2088 patients were invasively mechanically ventilated on the day of ICU admission and 1827 (87·5%) were invasively mechanical ventilated at some point during hospitalisation.
Infusion with sedatives while on mechanical ventilation was common: 1337 (64 %) were given benzodiazepines for a median of 7 days and 1481 (70·9%) were given propofol for a median of 7 days. Median Richmond Agitation–Sedation Scale score while on invasive mechanical ventilation was –4. 1704 (81·6%) of 2088 patients were comatose for a median of 10 days and 1147 (54·9%) were delirious for a median of 3 days.
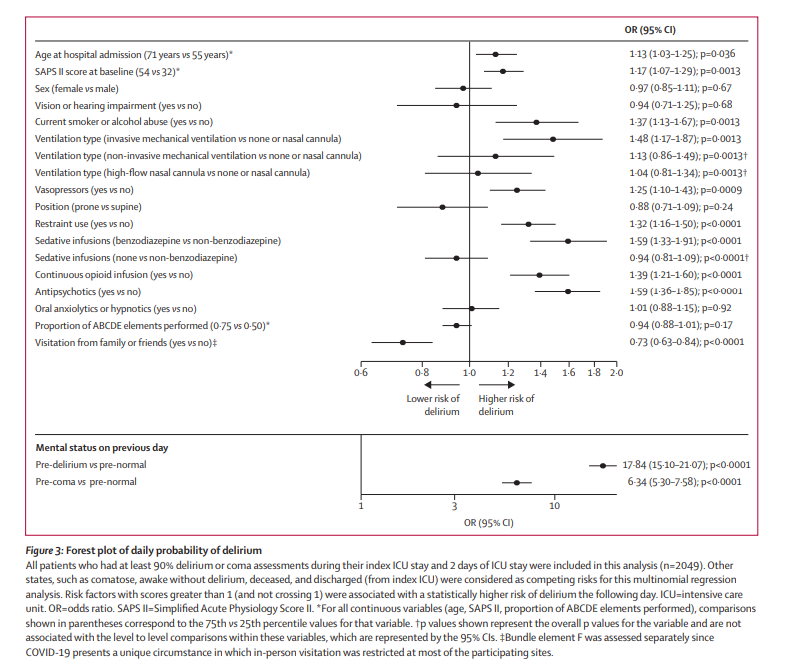
At baseline, older age, higher SAPS II scores, male sex, smoking or alcohol abuse, use of vasopressors on day 1, and invasive mechanical ventilation on day 1 were independently associated with fewer days alive and free of delirium and coma (all p<0·01). 601 (28·8%) patients died within 28 days of admission, with most of those deaths occurring in the ICU.
Acute brain dysfunction was highly prevalent and prolonged in critically ill patients with COVID-19. Benzodiazepine use and lack of family visitation were identified as modifiable risk factors for delirium, and thus these data present an opportunity to reduce acute brain dysfunction in patients with COVID-19.
In short, a new opportunity for humanization.
By Gabi Heras





{kind=link}
Leave A Comment