I have read with special attention and interest the editorial Humanizing the intensive care unit recently published in Critical Care by Wilson et at. First of all, I would like to congratulate the authors for inviting us to reflect on a topic that I consider as a priority for the development of an excellent management in intensive care units. If we would able to focus all our actions in the Dignity of people, health systems would probably be very different.
This topic has been the object of the interest and work of the research group that I lead, the international project for the humanization of the Intensive Care1 since the last five years. From the beginning, we found essential to listen not only to the patient as is intuited in the editorial, but also the experience of the other two stakeholders involved in ICU care: families and professionals. From our point of view, we cannot speak about humanization if the opinions, desires and needs of all actors are not taken into account. In addition, we all have the same problems in different parts of the world, so all people sensitive to this issue should work together looking for common solutions.
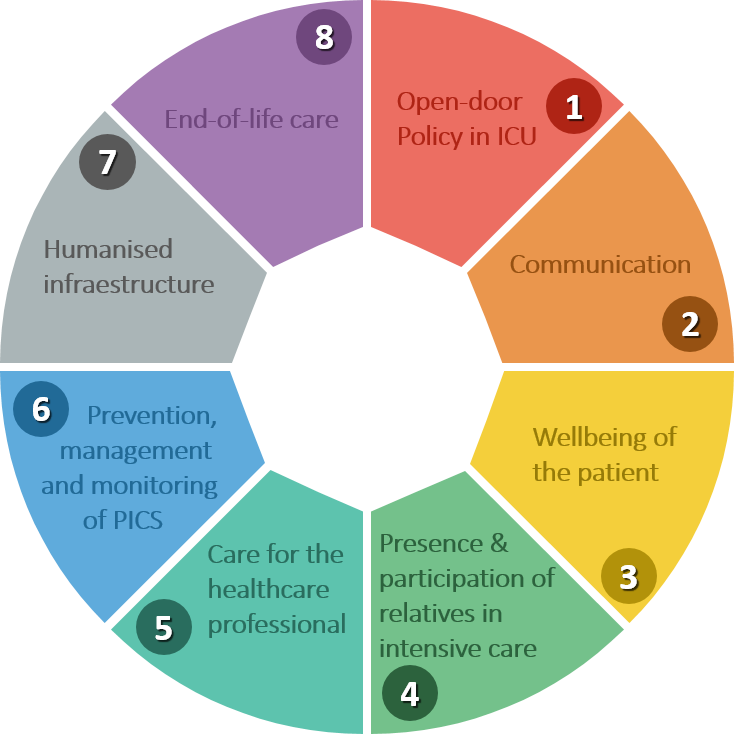
That’s why we picked up the opinions of over 10,000 people in February 2014, asking them what their ideal ICU would be like. We designed our eight research topics after that2, and this was the starting point to develop a global strategy to change the actual paradigm.
We think the humanization of intensive care medicine is a discipline of knowledge such as sepsis, mechanical ventilation or hemodynamic management, and we need a plan of action3 that involves an structured change of the way we work. This is a much deeper and more sustainable bundle than the only implementation of humanizing behaviours. As in all fields of knowledge, this change precises research projects – we have more than 70 articles published in last five years4– to scientifically demonstrate the benefit of humanization, as well as indicators that help us to measure what we do. For this reason, we elaborate in 2017 our handbook of good practices in humanization of intensive Care5, which consists of 159 tangible and measurable practices and whose compliance will transform the ICU into truly humanized spaces around the world, reducing social differences.
Some of the proposed actions want to improve the training of health professionals in non-technical skills. All that very importants things we have not been taught during our period at the University: active listening, empathy, compassion and communication. To this end, the project developed a training platform in these skills in 2016, called human tools6 as well as the first humanization of health care degree in conjunction with the Universitat de Barcelona, one of the most prestigious in the country7.
Therefore, Proyecto HU-CI members consider that speaking of humanization is not only a matter of good words. We need applied ethics and to move into action, with an exportable and reproducible method for any ICU in the world. Actually, this Project has the endorsement of 15 Scientific Societies of Intensive Care Medicine (SCCM included) and more than 50.000 followers.
By Gabriel Heras.
References
- Humanizing Intensive Care Proyect. https://proyectohuci.com/en/home/
- Heras La Calle, Gabriel. My Favorite Slide: The ICU and the Human Care Bundle. NEJM Catalyst. April 5th 2018
- Heras La Calle G, Alonso Oviés A, Gómez Tello V.A plan for improving the humanisation of intensive care units. Intensive Care Med. 2017 Apr;43(4):547-549.
- Scientific publications of Proyecto HU-CI: https://proyectohuci.com/es/publicaciones-cientificas/
- Grupo de trabajo de certificación de Proyecto HU-CI. Manual de buenas prácticas de humanización en Unidades de Cuidados Intensivos. Madrid: Proyecto HU-CI; 2017. https://proyectohuci.com/es/buenas-practicas/
- Training platform in Human Tools of Proyecto HU-CI: https://proyectohuci.com/es/campus/
- Humanization of Health Care Degree 2018-2019. https://proyectohuci.com/es/masterhumanizacion/






{kind=link}
Leave A Comment